Scottish National
BRACHIAL
PLEXUS
INJURY
SERVICE
Specialist multidisciplinary integrated management, assessment, surgical reconstruction and rehabilitation for brachial plexus injury in Scotland and the UK

We accept referrals from medical professionals.
Preferably patients should have been seen beforehand by an Orthopaedic Surgeon, Plastic Surgeon or a Paediatrician.
Allied Health Professionals are welcome to discuss cases with members of the team.
Completed forms can be posted or emailed to us.
If you prefer to send a referral by post please enclose as much relevant information to help us with a diagnosis. Recent imaging reports, neurophysiology reports, operation notes, muscle and sensory assessments and physiotherapy assessments are all useful.**
Post this information along with a referral form or cover letter to:-
SNBPIS
REH030 Ground Floor
New Victoria Hospital
Grange Road
GLASGOW
G42 9LF
**Referrals from within NHS Greater Glasgow & Clyde don't usually require this extra information.
Contact the on-call orthopaedic registrar on: 0141 201 1100 (QEUH switchboard).
Outside normal office hours urgent brachial plexus injury referrals are the responsibility of the on-call orthopaedic registrar at the Queen Elizabeth University Hospital.
The Adult Brachial Plexus Injury Service is based at the New Victoria Hospital in Glasgow. Outpatient clinics are held at the New Victoria Hospital in Glasgow. Outreach clinics are held twice a year at Woodend Hospital in Aberdeen. Surgery is performed at the Queen Elizabeth University Hospital and the Glasgow Royal Infirmary.
We welcome referral of any acute trauma patient with a brachial plexus injury. We can also advise on any peripheral nerve injury and admit as necessary. All patients must be assessed by the local trauma team.
The service employs:
The service has close ties with the University of Strathclyde's Department of Orthotics and Prosthetics.
Referrals are accepted from all over Scotland, from Northern Ireland and occasionally from the north of England. Referrals usually come from orthopaedic consultants, specialist registrars or general practitioners. Occasionally referrals are accepted from extended scope practitioner (ESP) physiotherapists, but this is usually with prior consultation.
Patients are assessed at the monthly brachial plexus clinics in Glasgow, the Aberdeen outreach clinics (spring and autumn), at a fracture or an orthopaedic clinic or, if necessary, on the ward as an emergency admission.
Surgery for adult patients is performed primarily at the Queen Elizabeth University Hospital in Glasgow with some procedures performed at the Glasgow Royal Infirmary.
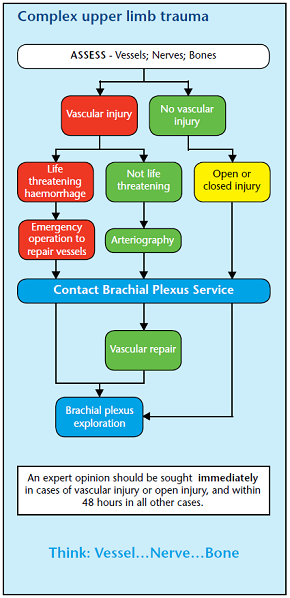
Acute: Resuscitate and stabilise the patient. Airway. Breathing. Circulation.
Radiographs - Chest/C-Spine
MRI of the C-spine or CT myelography. Both are useful in diagnosing root avulsions although neither is 100% accurate. MRI is easier to perform early after injury (see MRI Protocol at the bottom of this page).
CT of the cervical spine is useful in excluding cervical fractures and dislocations acutely. CT angiography is good when there is evidence of vascular injury.
Neurophysiology is not usually helpful in the acute situation.
The introduction of the National PACS means we can now access most imaging directly. It is therefore not usually necessary to send films or CDs with the patient. However we may not have access to radiology reports on PACS for investigations carried out in other hospitals. We would therefore be grateful if reports on MRI and CT scans could be sent with the referral.
MRI is most useful at defining nerve root avulsions (pre-ganglionic injury) or spinal cord damage. Imaging of damage to the post-ganglionic elements of the plexus is difficult to interpret. Therefore high resolution imaging of the C-spine from C3 to T2 is the priority.
Currently we use:
For brachial plexus injuries associated with dislocation of the shoulder, or other shoulder trauma, the nerve damage is usually below the level of the clavicle (infraclavicular). Therefore MRI of the C-spine is not necessary.
MRI of the shoulder is very useful particularly in diagnosing associated rotator cuff tears which may warrant early repair.
The following conditions are not included within the remit of the National Brachial Plexus Injury Service:-
Despite the name, brachial neuritis (lateral amyotrophy, Parsonage-Turner Syndrome) is not usually treated by the brachial plexus injury service. Patients with suspected brachial neuritis are frequently referred to our consultant team. In the majority of these cases treatment is not possible within the brachial plexus service and only general therapeutic advice can be given. Surgery has a limited role in management of this condition.
Vascular surgeons are able to treat this condition in some parts of Scotland. The consultants may be able to help outside the brachial plexus service remit and may be contacted to discuss individual cases.
Mr Timothy Hems
Consultant Orthopaedic Surgeon
0141 201 1100 (QEUH switchboard)
ggc.brachial.plexus@nhs.scot
Professor Andrew Hart
Consultant Plastic Surgeon
0141 211 4000 (GRI switchboard)
ggc.brachial.plexus@nhs.scot
SNBPIS Referrals
REH030
New Victoria Hospital
Grange Road
GLASGOW
G42 9LF
Contact the service administrator on:
0141 347 8916
ggc.brachial.plexus@nhs.scot
Nurse Specialist:
0141 347 8026
laura.falconer@nhs.scot
Occupational Therapist:
0141 347 8062
Lynsey.Warner@ggc.scot.nhs.uk
Specialist Physiotherapist:
0141 347 8685
andrea.shaarani@nhs.scot